Intussusception
Objectives
Upon finishing this module, the student will be able to:
- Recognize the signs and symptoms of intussusception.
- Understand the pathophysiology associated with untreated intussusception.
- Describe the evaluation and emergent management of intussusception.
- Discuss management options for intussusception.
Contributors
Update Authors: Kaylah Ibidapo, MD, and S. Margaret Paik, MD.
Original Author: S. Margaret Paik, MD.
Update Editor: Cosimo Laterza, MD.
Last Updated: June 2024
Introduction
Intussusception is a common cause of bowel obstruction in infants and young children. 80-90% of cases are children that are less than two years of age with a slight male predominance. Intussusception occurs when a portion of the intestine invaginates into itself. The proximal bowel segment (intussusceptum) telescopes into a distal bowel segment (intussuscipiens), pulling the connected mesentery with it, which is often referenced to as the lead point. This results in venous insufficiency and bowel wall edema. Necrosis and perforation of the bowel with peritonitis will ensue if left untreated. Unrecognized intussusception can be fatal.
There are multiple types of intussusception, with Ileocolic intussusception near the ileocecal junction being the most common. Other variations include ileo-ileo-colic, jejuno-jejunal, jejuno-ileal or colo-colic. Most cases are idiopathic without a known trigger or can be incited by a pathological lead point. Viral infections may be associated with intussusception, with one-third of patients having viral symptoms prior to an episode of intussusception. This is due to intestinal lymphatic tissue becoming stimulated, which can act as a lead point. Additionally, the incidence of intussusception increases during times of increased incidence of viral gastroenteritis. Additional causes of a lead point include Meckel’s diverticulum, tumors, polyps, duplication cysts, vasculitis, or vascular malformations. An identified lead point is more likely to be found in children older than two years old.
The classic presentation includes the sudden onset of colicky, intermittent abdominal pain. The pain is often episodic, with the child appearing well between episodes. Bloody stools and vomiting may also occur. Some patients may present with lethargy, listlessness, or a comatose appearance, which can lead to misdiagnoses such as sepsis, encephalopathy, or postictal states. An ill-defined, “sausage-shaped” mass can occasionally be palpated, though this is rare, and the absence of a palpable mass does not exclude the diagnosis.
The classic triad of abdominal pain, a sausage-shaped mass, and currant jelly stools (blood and mucus mixed with stool) is observed in only 15–20% of cases. Additionally, the absence of blood in the stool does not rule out intussusception. This diagnosis should also be considered in conjunction with other pathologies, such as vasculitic disorders (e.g., IgA vasculitis), viral gastritis, or oncologic abdominal masses.

Figure: Bloody stool in diaper.
The preliminary diagnostic studies include plain radiographic films of the abdomen and abdominal ultrasound. Potential findings on an abdominal x-ray include:
- Normal gas pattern.
- Intestinal obstruction with distended bowel and air-fluid levels.
- "Target" sign over the right kidney, consisting of two concentric radiolucent circles.
- "Crescent" sign with a soft tissue density protruding into the gas-filled lumen of the large bowel.
- Paucity of air in the cecum.
- Signs of perforation with pneumoperitoneum (rare).

Figure: KUB x-ray revealing dilated loops of bowel with paucity of gas. Image courtesy of Frank Gaillard. Used under the Commons Attribution-Noncommercial-Share Alike 3.0 Unported license.
Ultrasonography is the preferred diagnostic study for many clinicians. Its sensitivity and specificity approach 100% when performed by an experienced ultrasonographer. The classic ultrasound findings include a “bull’s eye,” “coiled spring,” or “target sign.” Additionally, ultrasound can identify a lead point in many cases of intussusception associated with underlying pathology. Color duplex imaging can also demonstrate a lack of perfusion and signs of ischemia.
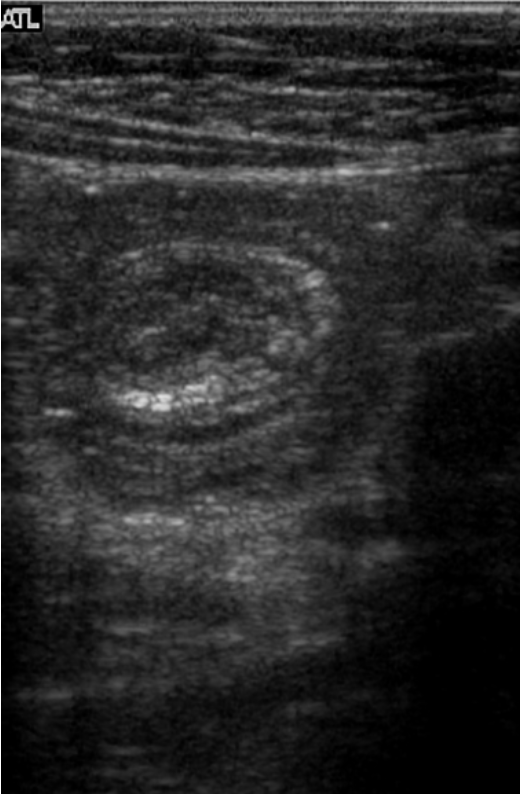
Figure: Target sign on ultrasound. Image courtesy of Behrang Amini. Used under the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported license.

Figure: Target sign and pseudo-kidney. Image courtesy of Tee Yu Jin. Used under the Creative Commons Attribution-Noncommercial-Share Alike 3.0 Unported license.
Intussusception can be seen on computed tomography (CT) as well but is not a preferred modality. CT is used when other radiographic studies are indeterminate or to better identify a pathological lead point.
Patients with evidence of bowel perforation require operative intervention. Patients without evidence of bowel perforation are managed with non-operative reduction using hydrostatic (barium, water-soluble contrast or saline) or pneumatic pressure enemas, guided by either fluoroscopy or sonography. Reduction is successful in 80-95% involving ileocolic intussusception with perforation risk of less than 1% for both hydrostatic and pneumatic pressure enemas. The choice of non-operative intervention depends on the radiologist and institution. Before undergoing enema reduction, patients require the following:
- Stabilization and adequate fluid resuscitation.
- Decompression of the stomach with placement of a nasogastric tube.
- Surgical consultation.
Patients are usually observed for 12-24 hours after successful non-operative reduction. Recurrence of intussusception is approximately 10% after non-operative reduction.
- Intussusception is one of the most common causes of bowel obstruction in children aged six months to three years, with most cases occurring under two years of age.
- Intussusception typically presents with sudden onset of episodic abdominal pain.
- Children may appear normal between episodes of bowel invagination.
- Bloody stools and vomiting are common associated symptoms.
- Some children may present with altered mental status, leading to misdiagnoses such as sepsis, encephalopathy, or a postictal state.
- Ultrasonography is the diagnostic method of choice for intussusception.
- Patients require stabilization, adequate fluid resuscitation, and placement of nasogastric tube prior to attempted reduction.
- Non-operative reduction is performed using either hydrostatic or pneumatic pressure enemas, guided by fluoroscopy or sonography.
- Surgical consultation should be conducted prior to non-operative reduction to prepare for cases of unsuccessful reduction or perforation during the procedure.
- Fallon SC, Lopez ME, et al. Risk Factors for Surgery in Pediatric Intussusception in the Era of Pneumatic Reduction. J Pediatr Surg. 2013 May.
- Freedman SB, Thull-Freedman J, et al. Pediatric Abdominal Radiograph Use, Constipation, and Significant Misdiagnoses. J Pediatr. 2014 Jan.
- Gray MP, Li SH, et al. Recurrence Rates After Intussusception Enema Reduction: A Meta-Analysis. Pediatrics. 2014 Jul.
- Jiang J, Jiang B, et al. Childhood Intussusception: A Literature Review. PLoS One. 2013 Jul 22.
- Lochhead A, Jamjoom R, Ratnapalan S. Intussusception in Children Presenting to the Emergency Department. Clin Pediatr. 2013 Nov.
- Mandeville K, Chien M, et al. Intussusception: Clinical Presentations and Imaging Characteristics. Pediatr Emerg Care. 2012 Sep.
- Territo HM, Wrotniak BH, et al. Clinical Signs and Symptoms Associated with Intussusception in Young Children Undergoing Ultrasound in the Emergency Room. Pediatr Emerg Care. 2014 Oct.