
Electrolyte abnormalities
Author Credentials
Author: Sharon Bord, MD/ Johns Hopkins University School of Medicine
Editor: William Alley, MD/ Wake
Section Editor: Matthew Tews, DO, Indiana University School of Medicine
Update: 2023
Case Study
A 52-year-old male presents to the Emergency Department after a missed dialysis session complaining of shortness of breath. He reports that he missed his last hemodialysis session due to feeling unwell.
Vital signs on Presentation are BP 150/90 HR 95 RR 18 POx 95% RA.
Pre-hospital EKG reveals a widened QRS complex.
Shortly after arrival to the ED patient goes into cardiac arrest with a PEA rhythm. You suspect the cardiac arrest is related to hyperkalemia. In this module you will focus on diagnosis and treatment for the most common electrolyte abnormalities that are seen in the ED.
Objectives
By the end of this module, the student will be able to:
Identify EKG changes associated with hyper- and hypokalemia.
Understand the different treatments for hyperkalemia and when to use each of them.
Identify EKG changes associated with hyper- and hypocalcemia.
Understand the treatment of hyper and hypocalemia.
Discuss common etiologies and clinical presentation of each of the above named electrolyte abnormalities.
Introduction
Electrolyte abnormalities are commonly present in patients who are seen in the emergency department. They are sometimes the reason for presentation, but more often are found when labs are checked for other chief complaints. It is important to consider electrolyte abnormalities for patients who present with altered mental status or delirium, shortness of breath or chest pain.
Initial Actions and Primary Survey
Certain electrolyte abnormalities can be life threatening while others are incidental findings that require only minimal treatment. It is important to be aware of the electrolyte abnormalities that require emergent or urgent treatments. The most worrisome complication of electrolyte abnormalities is developing an arrhythmia or cardiac arrest.
A key initial action when thinking about a life-threatening electrolyte abnormality is obtaining an electrocardiogram(EKG). One should focus EKG analysis on the length of the intervals, length of the QRS complex and T wave changes. Treatment decisions can sometimes be made based on the initial EKG alone.
The other focus should be on looking at past medical history for the patient. History of kidney failure, malignancy or cardiac issues can all be helpful when considering electrolyte issues. The patient’s history may help guide treatment for the patient as well.
Presentation
Hyperkalemia
Elevated potassium level is a common and life-threatening condition that is seen in the emergency department. Hyperkalemia is defined as a serum K of greater than 5.5 mmol/L. In order to reduce morbidity and mortality associated with this condition, early identification and treatment is key. It is important to recall that potassium is a primarily intracellular cation(lives mainly in the cell). When there is excess extracellular potassium, either from shifts or inability to excrete it, patients can experience arrhythmias and potentially cardiac arrest.
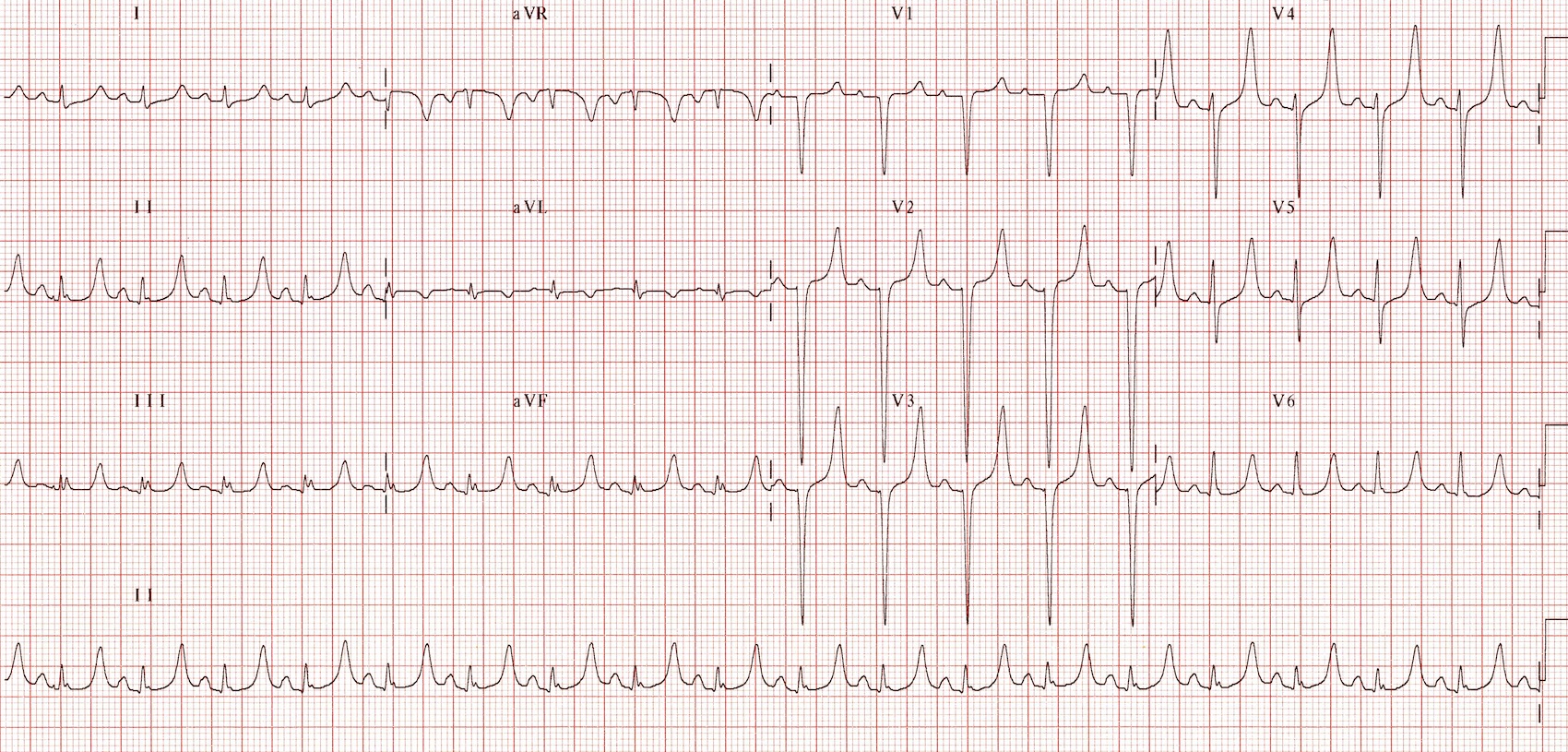
Note the peaked T-waves in this patient with a potassium of 7.0
Image 1. Image used under the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Based on a work at https://litfl.com. The original image is located on the following website: https://litfl.com/hyperkalaemia-ecg-library/
Performing an early EKG, especially in high-risk patients, and paying careful attention to changes consistent with hyperkalemia can be life saving. Patients who are at high risk include those on renal replacement therapy(peritoneal or hemo-dialysis), those with concern for diabetic ketoacidosis or patients with acute renal failure. EKG changes progress from peaked T-waves to widened QRS and eventually to ventricular tachycardia, fibrillation or pulseless electrical activity arrest. These progressive changes can correlate with rising potassium levels. For example, peaked T waves might correspond with a potassium level of approximately 6 mmol/L, whereas cardiac arrest generally occurs at higher levels.
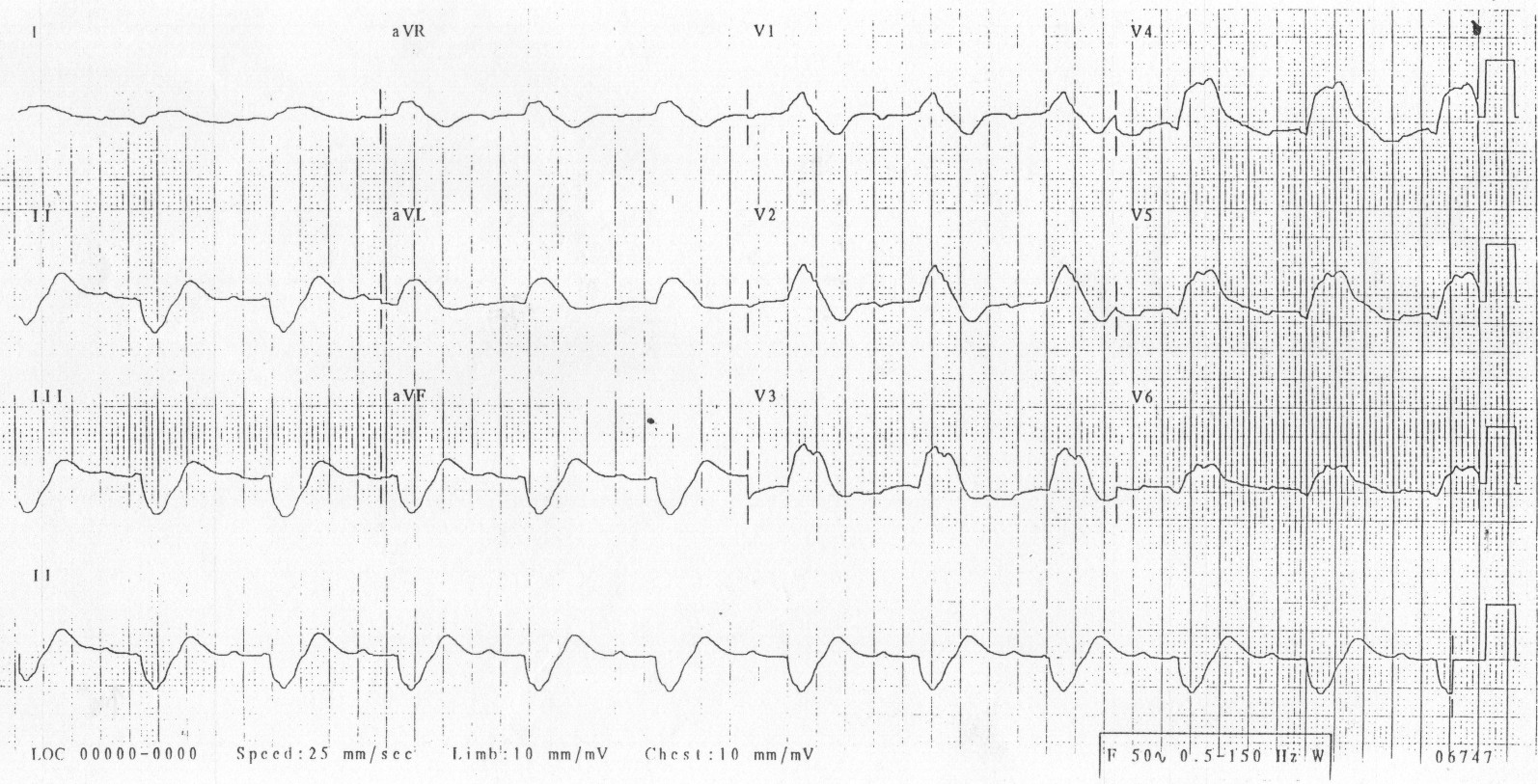
Note how the PR and QRS lengthen in hyperkalemia until the patient develops a “sine-wave” pattern EKG
Image 2. Image used under the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Based on a work at https://litfl.com. The original image is located on the following website: https://litfl.com/hyperkalaemia-ecg-library/
The most important initial treatment that should be administered if EKG changes are seen is administration of calcium gluconate or calcium chloride. Some emergency medicine practitioners advocate for calcium administration with peaked T-waves alone, while others will only treat it if additional findings are seen. The calcium will stabilize the cardiac membranes and, in turn, prevent further arrhythmias from developing. After the potassium level has been resulted, additional treatment to aid in shifting the potassium intracellularly includes insulin in combination with glucose, albuterol, or sodium bicarbonate. Additionally, total body excretion can be achieved using loop diuretics for patients who produce urine or potassium binders, such as sodium zirconium cyclosilicate. Ultimately dialysis treatments may be needed to treat hyperkalemia.
Hypokalemia
The EKG can also provide early indication of a low potassium level. Hypokalemia is defined as a potassium level less than 3.5 mmol/L, but EKG changes generally do not occur until the level goes below 2.7 mmol/L. Similar to elevated potassium levels, low potassium levels can cause myocardial arrhythmias and significant ectopy. EKG changes can include increased amplitude and width of P wave, T wave flattening and inversion, prominent U waves and apparent long QT intervals due to merging of the T and U wave. The U-wave is a deflection following the T wave. Hypokalemia causes enlarged and prominent T waves on the EKG. Potassium levels that are critically low (<1.7 mmol/L) can lead to torsades de pointes or“twisting of the points”, a polymorphic ventricular tachycardia.
Patients who have hypokalemia that is mild are oftentimes asymptomatic. As hypokalemia becomes more severe, muscle weakness, myalgias, paralysis and arrhythmias may develop. There are no classic physical exam findings that support the diagnosis of hypokalemia.

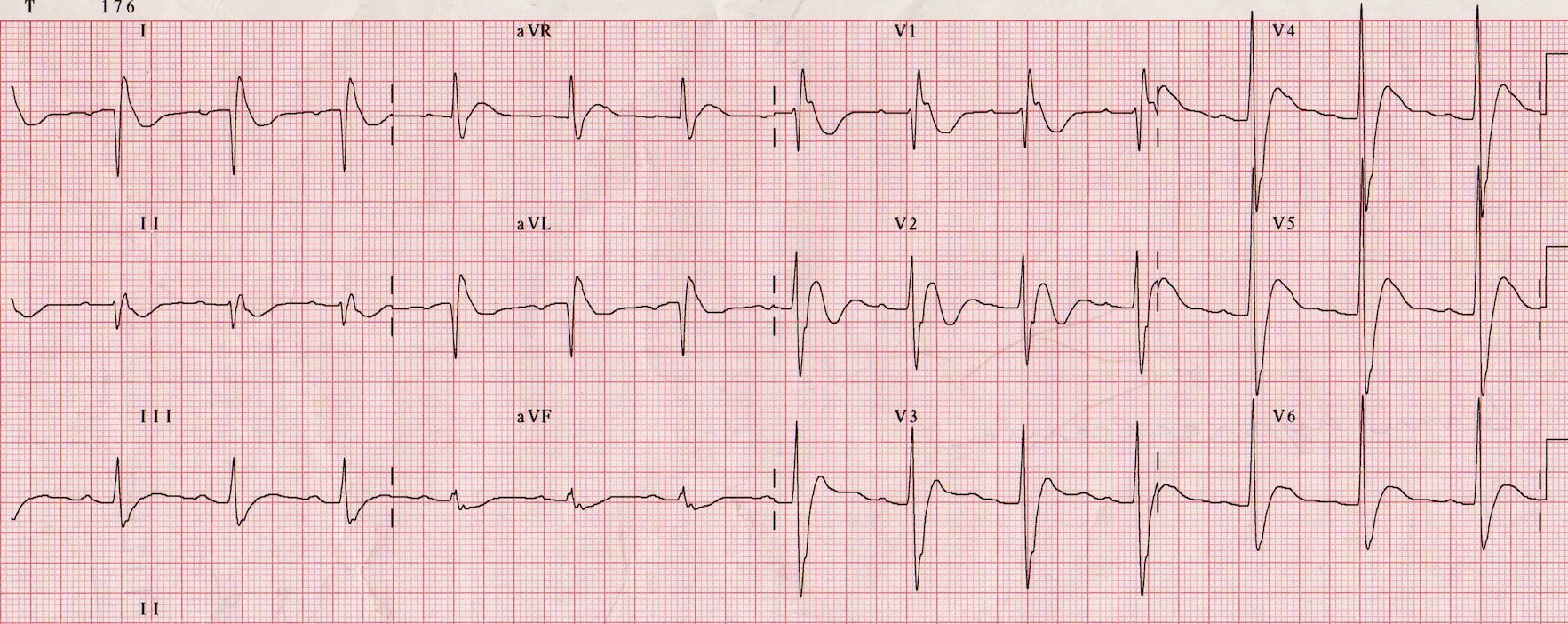
Patient with a potassium of 1.7
Image 3. Image used under the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Based on a work at https://litfl.com. The original image is located on the following website: https://litfl.com/hypokalaemia-ecg-library/
Hypokalemia can occur secondary to medications (common culprits include hydrochlorothiazide and furosemide), gastrointestinal loss, overzealous treatment for hyperkalemia or shifting of potassium into the cell. Hypomagnesemia is oftentimes associated with hypokalemia; thus it is important to check a magnesium level in any patient who presents with hypokalemia or arrhythmia.
Severe hypokalemia with EKG changes should be treated emergently with repletion with intravenous potassium chloride to a K of 4-4.5 mmol/L. Patients with mild or moderate hypokalemia can undergo repletion using oral agents as well. The magnesium level should be repleted as well to a level greater than 2 mmol/L. Of note, the potassium will not improve despite repletion unless the magnesium is within a normal range.
Hypercalcemia
Elevated calcium level is defined as a level greater than 2.7 mmol/L, with severe hypercalcemia being greater than 3.4 mmol/L. The most common EKG finding associated with hypercalcemia is shortening of the QT interval. In severe cases, Osborn or J waves might be seen or ventricular fibrillation might ensue. Recognition of these EKG findings can prompt urgent treatment.
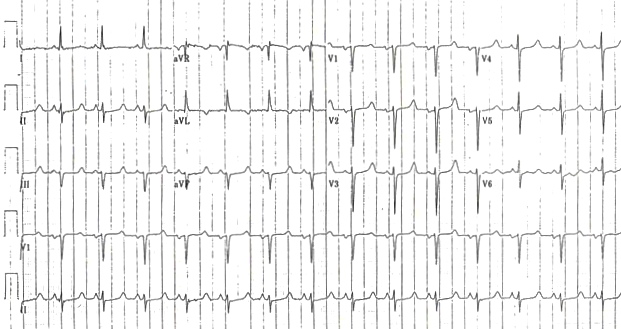
ECG in patient with hypercalcemia, the QT shortens
Image 4. Image used under the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Based on a work at https://litfl.com. The original image is located on the following website: https://litfl.com/hypercalcaemia-ecg-library/
Calcium homeostasis is a balance of bone absorption and reabsorption, parathyroid hormone and primarily renal excretion. Causes of hypercalcemia include hyperparathyroidism, myeloma, bony metastases, milk alkali syndrome, sarcoidosis or excess vitamin D intake. Emergent treatment to lower the calcium level include intravenous rehydration, loop diuretic or bisphosphonate administration. Further treatment once the EKG changes have resolved should be directed at correcting or treating the underlying cause.
Hypocalcemia
Chief complaints of patients who present with hypocalcemia include carpopedal spasm, neuromuscular excitability and, if severe, seizures might develop. In addition to obtaining an early EKG to support the diagnosis, Chvostek’s and Trousseau’s sign might also be tested. Chvostek’s sign is positive if the facial nerve is tapped at the angle of the jaw and twitching of facial muscles on the same side is noted. Trousseau’s sign is performed by inflating the blood pressure cuff to greater than the systolic BP for three minutes. In patients with hypocalcemia, they will have contraction and spasm of the muscles in their hand, wrist and fingers.
Patient with hypocalcemia, note the long QT interval
Image 5. Image used under the Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License. Based on a work at https://litfl.com. The original image is located on the following website: https://litfl.com/hypocalcaemia-ecg-library/
The most common finding on EKG in patients with hypocalcemia is a prolonged QT interval without any further changes. Hypocalcemia will rarely cause more serious cardiac arrhythmias, although atrial fibrillation might be found. Causes of a low calcium level include hypoparathyroid, low Vitamin D levels, acute pancreatitis and furosemide use.
Pearls and Pitfalls
- Electrolyte abnormalities are common in patients who present to the ED and may have life-threatening consequences. The initial screening EKG that many patients get may provide insight into the patient’s electrolytes and prompt emergent or urgent treatment.
- A careful history and physical exam can also provide clues to electrolyte abnormalities and their etiologies.
- Hyperkalemia is a common complication of renal disease, and when EKG changes are present, it is important to treat quickly to stabilize the cardiac membrane.
- Once recognized, it is important to treat critical electrolyte abnormalities to prevent arrhythmias and other complications.
Case Study Resolution
The patient was in a PEA arrest and, given the concern for hyperkalemia, was treated with Calcium chloride 1g IV, sodium bicarbonate, and insulin and D50. He regained a pulse shortly after medical administration. The lab calls and reports that the potassium level is 7.2 mmol/L.
Nephrology is consulted and the patient goes for emergency hemodialysis.
References
https://litfl.com/ecg-library/ (see above for individual references)
Pfenning C, Slovis C. Electrolyte Disorders, Rosen’s Emergency Medicine: Concepts and Clinical Practice. 114, 1525-1542.e2